Ultrasonography forms a key tool in monitoring patients with infertility. It mainly helps in monitoring the growth of the follicle (Egg in the ovary), its rupture and also to monitor the response of the endometrial lining in response to the egg growth and subsequently its release from the ovary. This basic procedure is done by transvaginal sonography(TVS), is a non invasive and cost effective method of determining ovulation. This facility in available at all fertility clinics and at certain sonography institutes and clinics and is called follicular study.
However some women have the fear of transvaginal sonography which is completely baseless. It is mainly psychological and we have seen that most of them get used to it as they proceed in their treatment. This is important because TVS gives more detailed and accurate information as compared to abdominal scan. Also it is many a times needed to do this scan when the women is menstruating and it is perfectly normal to do so.
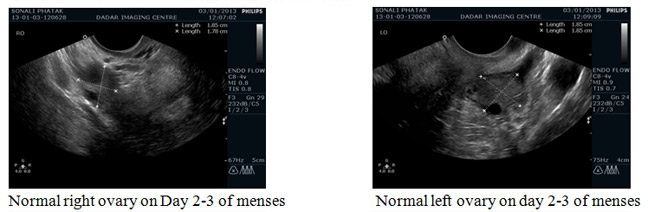
Two main things that are monitored in a follicular study are the ovaries and endometrium.
It is ideally started on the second or the third day of the periods when the woman is actually menstruating. The antral follicular count (AFC, number of eggs recruited in one particular cycle) is noted. This is an indirect method to detect the egg producing capacity in the woman. The ideal AFC is 3-6 eggs of size less than 10mm size in each ovary. Less means low egg producing capacity commonly seen in women above 30 years of age. More may indicate
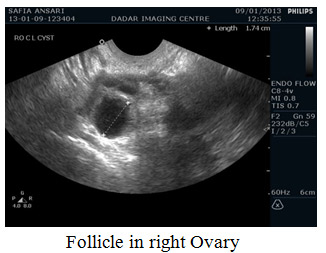
The woman may then be called directly on the 8-9 th day of the period and then every alternate day to monitor growth of follicle and then rupture. Growth of the follicle (egg) may occur in either left or right ovary in a particular cycle. There may be one or more follicles in a particular cycle. The optimum growth is between 18-20 mm after which the egg releases or ruptures as we call in medical language.
After the egg rupture the remnant in the ovary is called corpus luteum and this is then responsible for the endometrial growth (lining of uterus development). Corpus luteum is seen very well during follicular study. If the egg does not rupture, there is no corpus lutuem and this condition is called unruptured follicle. Some time an unruptured follicle may form a simple cyst in the ovary.
Documentation of rupture is important at it helps the doctor and the couple to time intercourse thereby improving pregnancy rates
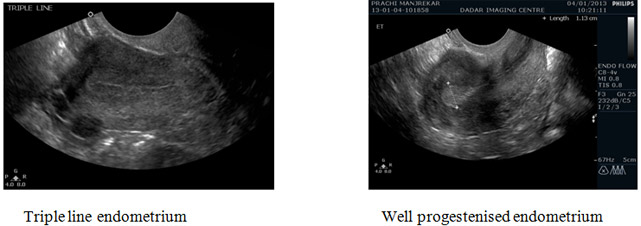
Another important factor to be studied during a follicular study is the endometrial lining and its growth along with the egg growth and release.
On the third day of cycle the endometrium is completely shed in menses and the lining therefore is thin. When the follicle or egg is growing the endometrial pattern is called triple line and the minimum thickness at the time of egg rupture should be 9mm or more. 5-7 days after ovulation the endometrium under the influence of corpus luteum prepares itself for implantation i.e. it prepares itself to receive the embryo (egg and sperm combine to form an embryo). The USG appearance of such endometrium is called progestanized endometrium.
The results of follicular study in terms of pregnancy rates can be improved in an infertile couple by giving medications or injections to facilitate egg growth and time the rupture. Sometimes a procedure called IUI (intra uterine Insemination) can be done at the time of rupture to improve pregnancy rates.
Follicular study also forms a basis if you need to undergo IVF or test tube baby centre treatment.
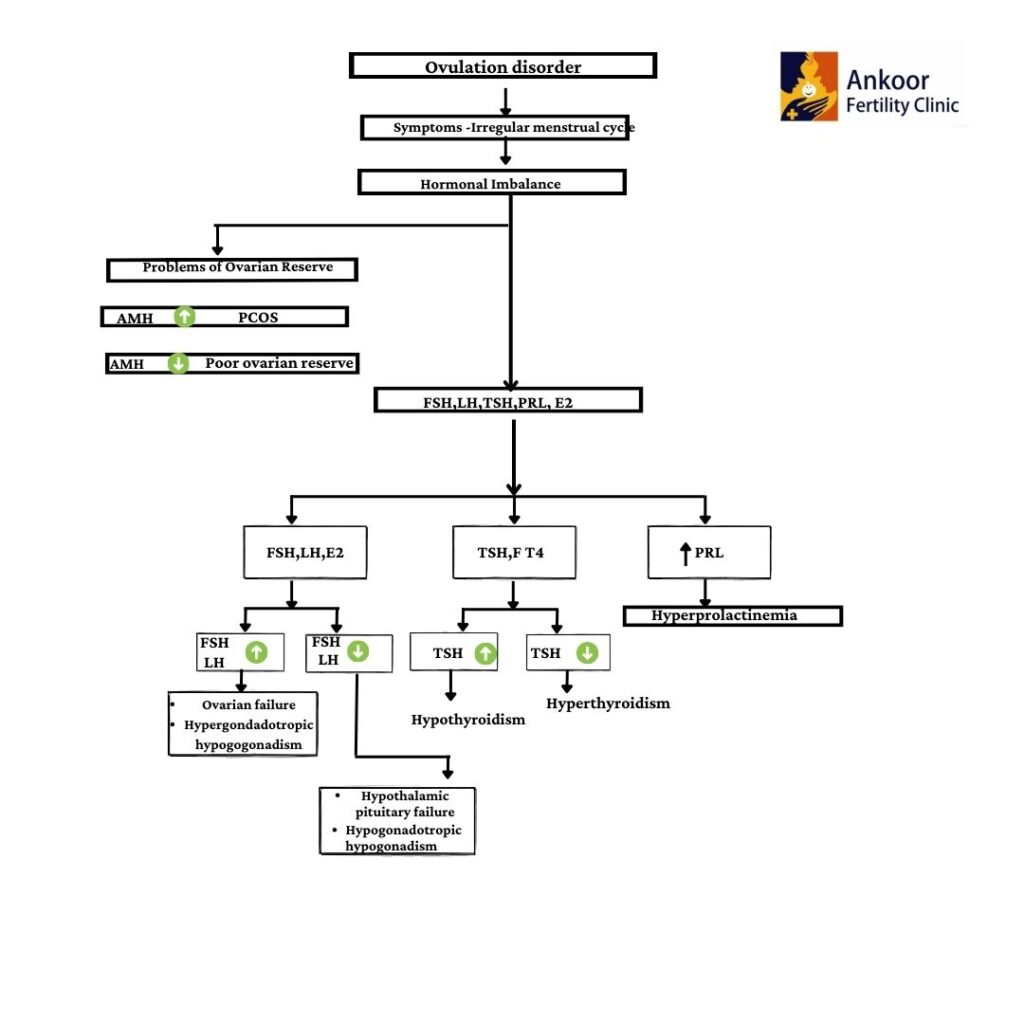
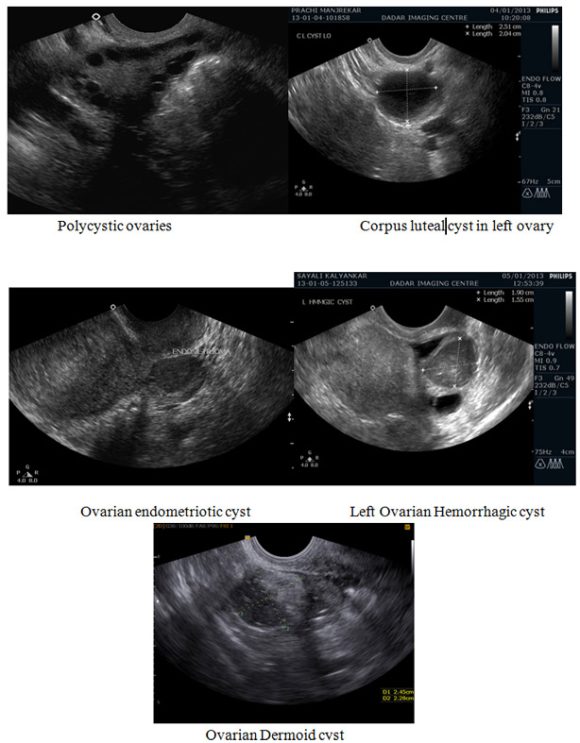
Ultrasonography mainly transvaginal can help in detecting the cause behind infertility in some cases. It can be useful in detecting:
Polycystic ovaries, Ovarian cyst (Endometrioma, Dermoid cyst, Simple cyst, corpus luteal cyst etc), Poor ovarian reserve, ovaries stuck to uterus as in PID.