




Locate fibroid and inject inj. Vasopressin in particular dilution with saline . This injection helps in reducing blood flow to fibroid ( by constricting the vessels supplying fibroid ). This is needed as fibroid is very vascular organ .
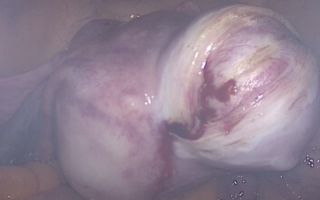
Taking incision on fibroid depending on type of fibroid.
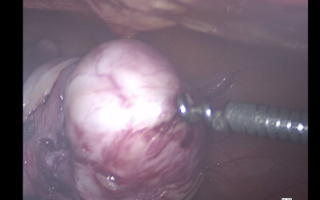
Inserting a screw like device ( myoma screw ) in fibroid to take out the fibroid from its capsule inside the uterus
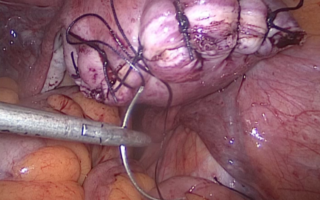
Suturing of uterus at the site from where myoma is removed ( myoma bed ) with absorbable suture material in 2 -3 layers

Removing the myoma outside the abdomen by use of special instrument called as morcellator. It uses mechanical energy to make small pieces of fibroids in the form of strips an then taken out of the abdomen through same incision.